
The hormone is used in the treatment of child growth deficit. Learn which signs to be aware of to diagnose the condition as soon as possible

Since the baby comes out of the womb, one of the parents’ main concerns is: is it growing as it should? For those who live with the child every day, however, it is difficult to solve this issue alone. Marking the height on the wall is fun, but it’s not enough when assessing your child’s growth.
The ideal is that the baby be taken early to the pediatrician and that the consultations are periodic, ranging between 4 and 6 months. Because each growth process is individual, only one expert can tell if the child’s development is within the parameters.
Nevertheless, adults should be aware of some signs that may indicate growth deficit, such as: height below the lower mean of the family channel, presence of predisposing conditions – such as tumors, genetic syndromes, radiotherapy in the region of head or babies born too small (around 43 centimeters) – and reduction in growth speed.

It is important to pay attention mainly if the child is growing less than 4 centimeters per year. For example, if she went to the pediatrician and the next visit grew only an inch. It may be normal, but it is necessary to look closely. Another sign can be observed in the child’s own school, noting the difference in height of the child in relation to others of the same age. We must suspect when the child is one of the lowest in the room – always remembering that those who are from the first semester are usually one of the youngest. But if you’re way below other children’s average, it’s important to look for a specialist to assess if everything’s okay.
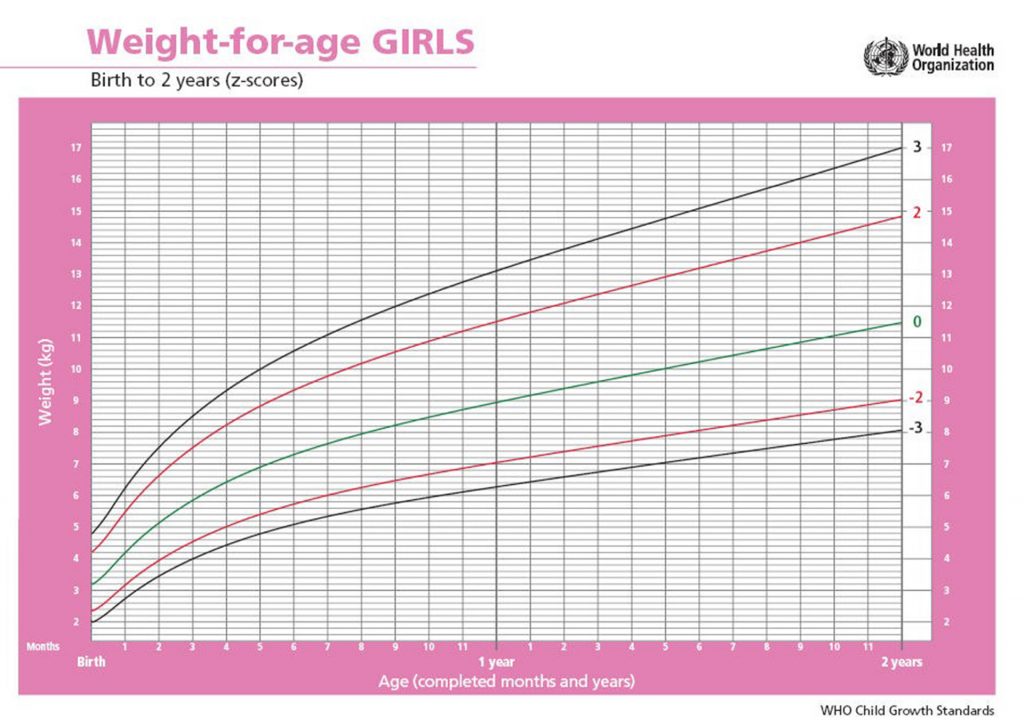
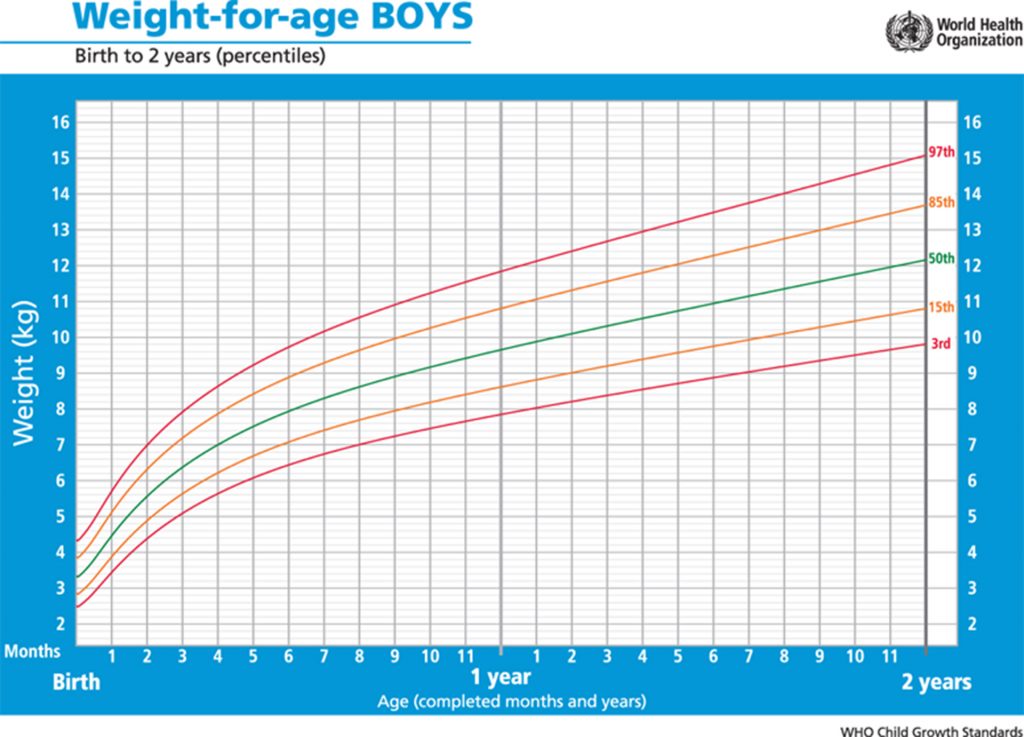
However, growth deficit can occur at any time in childhood, even when the child is one of the highest at any given time and then their growth rate becomes slower than normal. According to the growth curve of the World Health Organization (WHO), short stature is defined when the height of the person is below the 3rd percentile (growth reference 0 – 5 years).
That’s why regular visits to the specialist are so fundamental. The sooner the problem is diagnosed, the better the response to treatment, which is done by replenishing GH, the famous “growth hormone”.
The biological process of growth: fundamentals of importance for clinical practice

In general, growth is considered as an increase in body size and, therefore, it ceases with the end of the increase in height (linear growth). In a broader way, it can be said that the growth of the human being is a dynamic and continuous process that occurs from conception to the end of life, considering the phenomena of substitution and regeneration of tissues and organs. It is considered as one of the best indicators of child health, due to its close dependence on environmental factors, such as food, occurrence of diseases, general care and hygiene, housing conditions and basic sanitation, access to health services, thus reflecting the child’s living conditions in the past and present.
Family planning, adequate prenatal care, childbirth and puerperium, measures to promote, protect and recover health in the first years of life are crucial conditions for child growth to be processed in a way that healthy and adequate.
Factors that influence growth Growth is a biological process, of multiplication and increase in cell size, expressed by increased body size.
Every individual is born with a genetic potential for growth, which may or may not be achieved, depending on the living conditions to which from conception to adulthood. Therefore, it can be said that growth suffers influences from intrinsic factors (genetic, metabolic and malformations, often correlated, that is, they can be genetically determined) and extrinsic factors, among which stand out to health, hygiene, housing and general care for the child.
As a consequence, the conditions in which growth occurs, at every moment of the child’s life, including the intrauterine period, determine their chances of achieving their maximum growth potential, endowed with their genetic burden.
Regarding linear growth (height), it can be said that the final height of the individual is the result of the interaction between its load genetics and environmental factors that will allow greater or more expression of its genetic potential.
In children under five years of age, the influence of environmental factors is much more important than that of genetic factors for the expression of their growth potential. Genetic factors present their marked influence on the larger child, adolescent and young people.
Genetic inheritance
The property of living beings to transmit characteristics to descendants.
From the point of view of growth, the genetic inheritance received from the father and mother establishes a potential or target that can be achieved.
Few biological functions depend so much on genetic potential growth. However, at any time, from conception and especially in young children, environmental factors can disturb the pace and quality of this process. The scope of this biological goal depends, in fact, on the conditions of the environment where the growth of the child occurs being its marked influence.
There are large individual variations in growth potential given by genetic inheritance. It is observed, for example, that the variation of the adult population, healthy, male is about 20 cm, while this same variation between siblings is 16 cm and among homozygotic twins is 1.6 cm.
Influence of the genetic factor on growth
Normal genetic variability is always taken into account when diagnoses of growth deficit are made. The influence of the genetic factor on growth can be demonstrated through several examples:
• In linear growth:
The correlation coefficient between the height measurements of the parents and the height/length of the children at different ages: at birth this coefficient is 0.2, because the growth of the newborn reflects more intrauterine conditions than the fetal genotype. This coefficient rises rapidly, so that at 18 months it reaches 0.5, which is approximately the value it will have in adulthood. From 2 to 3 years to adolescence, the correlation of the parent/child height can be used to predict patterns for the height of children, in relation to the height of their parents.
The correlation coefficients between the height measurements of a child at successive ages and their own height in adulthood: this correlation of length at birth with height in adulthood is 0.3, rising rapidly so that from 2 to 3 years its value is 0.8. The practical implication of this relationship is that the height in adulthood can be estimated from the height of 2 to 3 years with an approximate error of up to 8 cm. At puberty, this correlation decreases because some children mature earlier and others later, but if bone age is taken into account it is possible to make the prediction.
The low correlation coefficient observed in the first years of life possibly reflects the great influence that the environment exerts on this phase of growth, minimizing the correlation with genetic potential. As the child gets older, the influence of the environment is attenuated, gaining importance to genetic factors.
The influence of the environment
The influence of the environment occurs since intrauterine life,
when growth is limited from a certain moment by the intrauterine cavity space, until adulthood.
Habicht, in 1974 (Ref. 1), demonstrated that children under 5 years of various nationalities, grow at a similar pace (the exception of the Eastern and some African tribes), provided that they are subjected to good living conditions. The same does not happen with children of the same nationality, but under different socioeconomic conditions (high-level conditions grow similarly to children from developed countries, while those with low socioeconomic status grow at a slower pace).
Increasingly, there is evidence on genetic uniformity of the human species and the increasing weight of other constraints, favoring or preventing the expression of genetic potential.
It was also proved that children of Japanese immigrants who were born and lived in the United States were taller than their patricians who remained living in Japan. Currently, with the development achieved by Japan, this difference has disappeared, thus evidencing the great influence that environmental factors exert on the secular trend of population group growth.
It is important to note that the younger the child, the more dependent and vulnerable the environment is. This causes favourable conditions for growth are a function, not only of the material and institutional resources with which the child can count (food, housing, sanitation, health services, day care centers and preschools), but also of general care, such as time, attention, affection that the mother, family and society as a whole dedicate to him.
Time, attention and affection define the quality of child care and, when maximized, allow the optimization of the material and institutional resources available to the child.
In a study with 300 pairs of separately created homozygous twins, and in very different socioeconomic conditions, an average variation of 6 cm in height was observed as adults, and individuals raised in poor environments with limited access to health actions were always lower than their siblings (Ref. 2).
Intrauterine growth and birth weight
The period of intrauterine growth is of vital importance to humans. That’s when you see higher growth speed. An idea of this speed can be illustrated by the following facts: in the short period ranging from conception to the moment of implantation in the uterus, the egg has several cell divisions, so that when implanting, it already has 150 cells. At the end of the 8th week after fertilization (about the 12th week of gestation), the embryonic period ends and the conceptus already presents the human form with arms and legs, a heart that beats and a nervous system that shows signs of onset of reflex responses to tactile stimulus (Ref. 3).
It is in this period, with higher growth rate, that external risks (ifneccious agents, maternal malnutrition, use by the mother of tobacco and other drugs, insufficient placental irrigation, maternal diseases, among others) of aggression to the fetus are larger, more severe and with more generalized repercussions.
In the clinical examination of pregnant women, the height of the bottom of the uterus for gestational age is one of the important measures to assess the growth of the fetus. Its standardized, serial and compared measurement with a weight growth pattern for gestational age (Ref. 4) allows detecting at-risk children. Values below the 10th percentile of the reference increase by 3.5 % the risk of intrauterine growth retardation. The association of uterine height with maternal weight gain during pregnancy has a sensitivity of 75% to predict small babies for gestational age. In the case of these two indicators presenting values below standardized limits as normal, the pregnant woman should be referred to a level of greater care complexity (Ref. 4).
Birth weight
The indicator that best portrays what occurs during the fetal phase is the birth weight of the child. Birth weights less than 2,500 g may be due to prematurity and/or intrauterine growth deficit. Newborns under 2,500 g are generically classified as low birth weight.
Several factors can negatively influence intrauterine growth, and in brazil, the most important are: smoking, alcohol and other drugs, arterial hypertension, chronic infectious diseases, sexually transmitted diseases, the nutritional status of pregnant women, the short interpartal interval (less than two years), high parity, maternal age (<19 years and >35 years), multiple pregnancy and congenital anomalies. For this reason, they are called risk factors for low birth weight (<2,500g).
Many of these factors have socioeconomic causes and can be prevented with good coverage by health services and prenatal control. Babies of low birth weight may be only premature babies, thus classified because they did not complete their normal gestation time and, therefore, their intrauterine growth, being called babies with adequate weight for gestational age (GAA). However, they may also be full-term infants (=>37 weeks) who did not have good growth in the uterus, i.e., they have growth retardation, being called small for gestational age (SGA).
Premature babies may also occur small for gestational age. Other babies may be large for their gestational age (GIG), as occurs with babies who are children of diabetic mothers.
Although every child weighing less than 2,500 g is considered as at risk, premature babies (born less than 37 weeks of gestation) whose weight is suitable for gestational age (GAA) have a better prognosis (excluding those of less than 37 weeks of pregnancy) whose weight is suitable for gestational age (GAA) has a better prognosis (except those of less than 1,000 g), especially those living in favorable environmental conditions. Such children have compensatory postnatal growth, reaching normal weight for age still during the 1st year of life (Ref. 5). This compensatory growth is a phenomenon that occurs in response to a slowdown in the rate of normal growth. Fixed the cause, and if environmental conditions are adequate, the body begins to grow at a higher rate than expected for age. This is a phenomenon widely found in malnourished children in the recovery phase.
Small babies for gestational age (SGA), preterm or full-term births, tend to remain small for age or even malnourished, requiring special attention from child care services.
In terms of Public Health, it is recommended to intervene with the objective of working on the prevention of low birth weight, investing in good coverage and prenatal care (Ref. 5).
REFERENCES
HABICHT, J.P. et al. Height and weight standards for preschool children.
How relevant are ethnics differences in growth potencial? Lancet, n. 1,
p. 661-4, 1974.
TANNER, J.M. Growth e Development. 2ª edição de Frank Falkner
and Tanner. Ney York, London: J.M. Ed. Plenum Press, v. 2, 1960.
TANNER, J.M. Foetus into Man: Physical Growth from Conception
to Maturity. London: Open Books, 1978.
BRAZIL. Ministry of Health, Pan American Health Organization.
Ten Steps to Healthy Eating, Food Guide for
children under 2 years. Brasilia, 2002.
BURGESS, H.J.L.; BURGESS, A.P. A modified standard for mid-upperarm circumference in young children. Journal of Tropical Pediatrics,
n. 15, p.189-192, 1969.
Disclaimer: This post may have affiliate links.